Blog
Learning Materials
Female Hairline Transplant: What Women Need to Know
Updated: May 20, 2026
TL;DR:
- Women with diffuse thinning face limited surgical options, with only 2–5% qualifying for hair transplants. Techniques like DHI offer natural results without full head shavings, and careful design ensures a feminine, soft hairline. Non-surgical treatments such as minoxidil and spironolactone are often more suitable for most women seeking hair restoration.
If you're noticing your hairline thinning or receding, you're far from alone. A female hairline transplant can restore density and shape where hair loss has changed your appearance, but the path to surgery is more selective for women than most people realize. Female hair loss affects around 40% of women by age 50, yet the surgical options, candidacy rules, and design considerations differ significantly from what men experience. This guide walks you through everything you need to know before making any decisions, from whether you qualify to what realistic results actually look like.
Table of Contents
- Key takeaways
- Female hairline transplant candidacy explained
- Techniques used in a ladies hair transplant
- Hairline design for female hair implants
- Recovery and results: what to expect
- Non-surgical options when surgery is not the answer
- My honest take after working with female transplant patients
- Start your hair restoration with Myhair
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Candidacy is rare | Only 2–5% of women with hair loss qualify for surgical restoration due to diffuse thinning patterns. |
| Technique matters | DHI is preferred for women because it allows transplantation without shaving the entire head. |
| Design is art | Soft, irregular hairlines built with single-hair grafts at acute angles produce the most natural results. |
| Recovery takes time | Expect shock loss around weeks 6–12 and full density results after 12–18 months. |
| Non-surgical options exist | Most women are better served by minoxidil, PRP, or spironolactone before considering surgery. |
Female hairline transplant candidacy explained
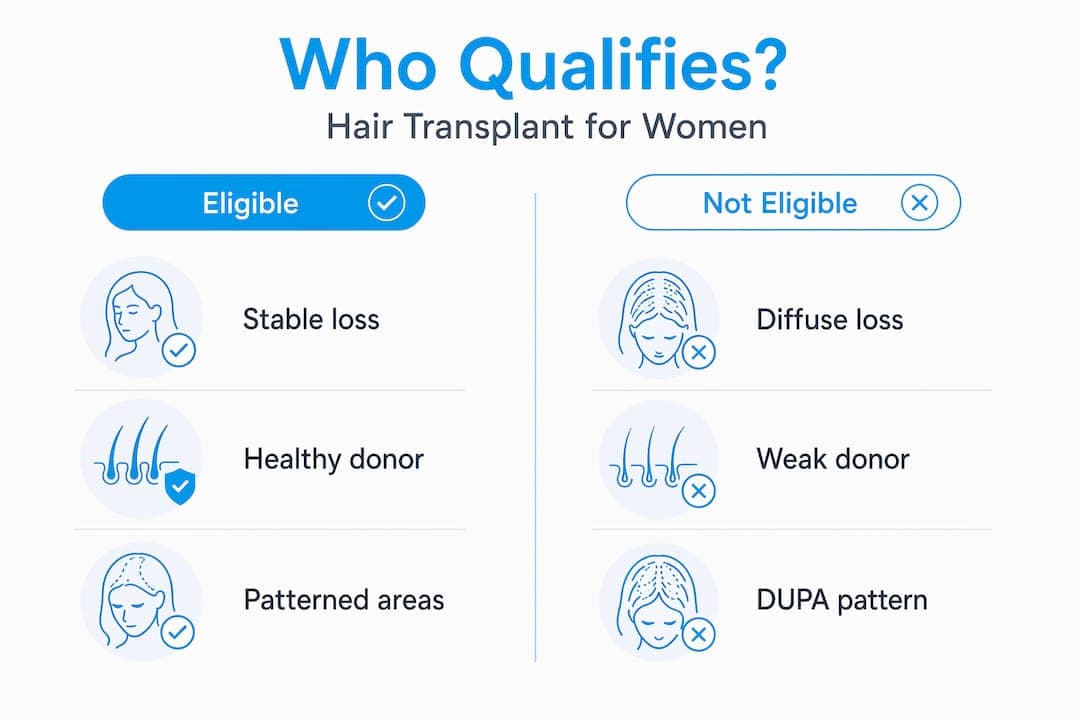
Before you research clinics or costs, you need to understand whether you're actually a surgical candidate. This is where many women get blindsided. The reality is that only 2–5% of women experiencing hair loss qualify for surgical hair restoration. That number is not a typo. Compare that to roughly 90% of men with hair loss who are surgical candidates, and you start to see how fundamentally different this process is for women.
The reason comes down to hair loss patterns. Men typically experience patterned baldness with a stable donor zone at the back and sides of the scalp. Women more often experience diffuse thinning, where hair thins across the entire scalp rather than in a clearly defined region. When the donor zone is also thinning, transplanted follicles may not survive long term.
Women with Diffuse Unpatterned Alopecia (DUPA) face a particularly challenging situation. DUPA patients have compromised donor follicles across the scalp, which means grafts extracted from that area carry miniaturized hair that will likely continue to thin after transplantation. Placing those follicles into a new location does not make them healthy again.
Common causes that affect candidacy
Understanding why your hair is thinning shapes everything about your treatment path. The most common causes a surgeon will evaluate include:
- Androgenetic alopecia (female pattern hair loss): Follows the Ludwig scale, with thinning concentrated at the crown and part line
- Traction alopecia: Caused by years of tight hairstyles pulling at the hairline, often leaving intact donor zones, which makes these patients better candidates
- Hormonal imbalances: Thyroid dysfunction, elevated androgens, and post-pregnancy shifts can all trigger temporary or progressive loss
- Autoimmune conditions: Alopecia areata creates patchy loss that is typically not treated surgically
- Nutritional deficiencies: Iron, ferritin, and vitamin D levels directly impact follicle health
A thorough diagnostic workup before any surgery should include blood panels, trichoscopy (scalp imaging), and a pull test to assess active shedding. Untreated hormonal or autoimmune causes can worsen outcomes even after a technically successful transplant, which is why medical clearance is non-negotiable. You can learn more about the full spectrum of female hairline causes and solutions to better understand your own pattern before booking a consultation.
Techniques used in a ladies hair transplant
Once a surgeon confirms you have a stable donor area and a treatable pattern, the next question is which technique fits your anatomy and lifestyle. Three main methods are used in a ladies hair transplant, and they are not interchangeable.
| Technique | Scarring | Shaving Required | Best For Women |
|---|---|---|---|
| FUE (Follicular Unit Extraction) | No linear scar | Partial shave | Most female candidates |
| DHI (Direct Hair Implantation) | No linear scar | Minimal to none | Women wanting no visible shaving |
| FUT (Follicular Unit Transplantation) | Linear scar at donor site | Full donor strip | Rarely recommended for women |
FUE extracts individual follicular units one by one from the donor zone. FUE leaves no linear scar, making it appealing for women who wear their hair up or short. A partial shave of the donor area is usually required, but surrounding hair can cover it during recovery.

DHI takes the process a step further. Using a specialized implanting pen called a Choi implanter, grafts go directly into the recipient area without pre-made incisions. DHI enables graft implantation without shaving the entire head, which addresses one of the biggest cosmetic concerns women bring to consultations. You walk out of the procedure with your existing hair largely intact and no obvious signs of surgery to your social circle.
FUT involves removing a strip of scalp from the donor area, dissecting it into individual grafts, and implanting them. It does allow for a higher graft count per session, but the linear scar it leaves makes it a poor fit for most women. Sessions across all techniques typically involve 1,500 to 3,500 grafts and last between 4 and 8 hours, usually completed in a single day.
Pro Tip: Ask your surgeon specifically whether DHI is available at their clinic and whether they have experience performing it on female patients without full head shaving. Not all clinics offer this option, and experience with female cases makes a significant difference in outcomes.
Hairline design for female hair implants
The surgical technique is only half the picture. For female hair implants, the design of the hairline itself is where artistry separates good results from truly natural ones. A woman's hairline is fundamentally different from a man's, and designing one requires a different eye entirely.
Female hairlines tend to be rounded and softer, with a natural irregularity at the front edge. There is no sharp, defined border. Instead, the transition from forehead to hairline is gradual, with fine, wispy strands creating a feathered look rather than a hard line. Replicating that in surgery is genuinely difficult.
Single-hair grafts placed at 10–15 degree angles mimic the way natural frontal hair emerges from the scalp at an acute, forward-facing angle. Using multi-hair grafts or placing them too upright at the hairline is what creates the "pluggy" or doll-like appearance that has become shorthand for a bad transplant.
Key design priorities your surgeon should discuss with you:
- Facial proportions: The ideal female hairline sits roughly 6–8 cm above the brow, but this varies with forehead height and face shape
- Soft frontal fringe: The leading edge should use only single-hair grafts to create a natural transition
- Temple area restoration: Women often lose hair at the temples first, and restoring soft temple points can dramatically rejuvenate the overall framing of the face
- Part line density: Thinning along the central part is one of the most visible signs of female pattern loss and a key area for targeted density restoration
Pro Tip: Bring reference photos of your own hairline from 10 years ago to your consultation. Surgeons who design hairlines using your historical photos rather than a generic template produce far more personalized and satisfying results.
You can explore the detailed differences in female hairline patterns and care to understand how your specific type shapes the design approach.
Recovery and results: what to expect
Setting realistic expectations before surgery protects you emotionally and physically. The recovery from a female hairline correction procedure follows a predictable arc, but knowing each phase in advance makes the harder stretches much easier to handle.
- Days 1–5: Mild swelling around the forehead and donor area. Scabbing appears at graft sites. Sleep with your head elevated and avoid touching the recipient zone.
- Days 7–10: Most patients can return to desk work and light daily activities. Redness begins to fade. Scabs start to fall naturally.
- Weeks 2–4: Transplanted hairs begin to shed. This is expected and does not mean the grafts have failed. The follicle is still alive beneath the scalp.
- Weeks 6–12: Shock loss typically occurs in this window, which is the temporary shedding of native hairs near the transplant zone triggered by surgical trauma. For women, longer existing hair often camouflages this phase effectively.
- Months 4–6: New growth begins emerging. Hair is often fine and uneven at first. Patience is critical here.
- Months 12–18: Full results are visible at the 12–18 month mark, when transplanted follicles have fully cycled and reached mature thickness.
"The transplant improves what you have. It does not restore the hair density of your twenties. Pairing surgery with ongoing medical treatment is what produces lasting, satisfying results."
One thing many women underestimate is the emotional weight of the "ugly duckling" phase between months two and four, when hair looks patchy and the new growth has not yet appeared. Having a surgeon or care team who prepares you for this window genuinely matters.
Non-surgical options when surgery is not the answer
Because most women do not qualify for the best hair transplant for women (surgical route), understanding your non-surgical options is not a consolation prize. For many women, these treatments produce real, lasting results without any of the surgical risk or recovery time.
- Minoxidil (2% or 5% topical, or oral): The most widely used treatment for female pattern hair loss, shown to slow loss and stimulate regrowth in many women with consistent use
- Spironolactone: An antiandrogen medication that can produce 21–28% improvement in hair count in female pattern loss, with response rates up to 75% in women with elevated androgens
- PRP (Platelet-Rich Plasma) injections: Concentrated growth factors from your own blood are injected into the scalp to stimulate follicle activity, often used as a standalone treatment or alongside surgery
- Low-level laser therapy (LLLT): FDA-cleared devices and in-clinic treatments that use red light wavelengths to energize hair follicles and reduce shedding
- Scalp micropigmentation (SMP): A cosmetic tattooing technique that creates the appearance of density and a defined hairline without any actual follicle transplantation
Pro Tip: Before booking a surgical consultation, spend six months on a medically supervised treatment plan. If your hair loss stabilizes or improves, you may not need surgery at all. If it progresses despite treatment, you have a much clearer picture of your pattern and candidacy.
Addressing underlying causes matters as much as the treatment itself. Correcting thyroid levels, improving iron stores, or changing tight hairstyling habits can halt active loss and create the stable environment that either a medical or surgical treatment needs to work. Visit Myhair's guide on hair growth treatment for women for a deeper look at how to stack these approaches effectively.
My honest take after working with female transplant patients
I've worked alongside enough surgeons and patients to say this clearly: the most common mistake I see women make is not being given an honest candidacy assessment early enough. A consultation that ends with "you're a candidate" without a full hormonal workup, trichoscopy, and a real conversation about your hair loss stability is a consultation that is rushing past the most important step.
The other thing that strikes me every time is how much the artistic quality of hairline design varies between surgeons. Two surgeons using the exact same DHI technique on similar patients can produce dramatically different results. The surgeon who understands the feathered, soft architecture of a feminine hairline will always outperform one who applies a male-pattern template.
I've also seen the emotional side of recovery reshape how women feel about the decision entirely. The patients who were prepared for the ugly duckling phase, who understood shock loss was temporary and that results take over a year, came through the process with their confidence intact. The patients who were not prepared for it often experienced deep regret at the four-month mark, even when their final outcome was excellent.
My honest advice: be skeptical of any clinic that minimizes the difficulty of female candidacy, rushes the design conversation, or can't show you a portfolio of female-specific results. The best outcomes come from surgeons who treat your case as the specialized, nuanced procedure it actually is.
— Cyriac
Start your hair restoration with Myhair
Understanding how to fix your female hairline starts with knowing exactly what you're dealing with. Not all hair loss is the same, and the difference between a pattern that responds to medication and one that requires surgery is not always visible to the naked eye.

Myhair's AI-powered hair analysis scanner gives you a detailed assessment of your scalp and hair health using your phone camera, providing the kind of personalized insight that typically requires a clinic visit. Whether you're tracking changes over time, preparing for a surgeon consultation, or exploring treatment options for the first time, Myhair helps you understand your scalp's current state with precision. You can also use the hair analysis onboarding to get started with a structured, guided approach to tracking your restoration progress.
FAQ
Who is a good candidate for a female hairline transplant?
Women with stable, localized hair loss (such as traction alopecia or a clearly receded hairline) and a healthy donor zone are the strongest candidates. Only about 2–5% of women with hair loss qualify for surgical restoration, making thorough pre-surgical evaluation critical.
What is the best hair transplant technique for women?
DHI (Direct Hair Implantation) is widely preferred for women because it allows graft implantation with minimal to no shaving of the recipient area, preserving cosmetic appearance during and after the procedure.
How long does it take to see results from a female hairline correction?
Initial growth appears around months 4–6, but full, mature results from a female hairline correction take 12–18 months to develop as transplanted follicles complete their growth cycles.
Can women with diffuse hair loss get a transplant?
Women with Diffuse Unpatterned Alopecia (DUPA) are generally not good candidates because their donor follicles are also affected by miniaturization, which means transplanted grafts are likely to continue thinning over time.
What non-surgical options work best for women who are not transplant candidates?
Minoxidil, spironolactone, PRP injections, and low-level laser therapy are the most evidence-backed options. Spironolactone in particular shows up to 75% response rates in women with elevated androgens, making it a strong first-line treatment before considering surgery.